Allergic rhinitis (AR) is highly prevalent in Singapore. It occurs in about 40% of our population, making the prevalence of AR in Singapore amongst the highest in the world It is also strongly associated with asthma and both conditions often coexist One-third of AR patients suffer from asthma while three-quarters of asthmatics have moderate to severe AR Uncontrolled moderate to severe AR also often results in poor asthma control.
SYMPTOMS OF AR
Classical symptoms of AR include nasal obstruction, rhinorrhea, sneezing and nasal itch. Other symptoms include throat irritation, post-nasal drip and cough. Ocular symptoms such as eye itch and tearing (allergic conjunctivitis) are also not uncommon.
SENSITISATION PATTERNS
In Singapore, sensitisation to house dust mites (HDM) is present in 70 to 80% of the population More than 90% of Singaporeans with AR and/or asthma are sensitised to the HDMs (Dermatophagoides pteronyssinust Dermatophagoides farina and Blomia tropicalis) It has been shown that residency in Singapore increases HDM sensitisation as well.
ALLERGIC RHINITIS IS NOT A TRIVIAL CONDITION
While AR is not associated with severe morbidity and mortality, it significantly decreases one's quality of life and impairs quality of sleep which resulting in irritability, fatigue and decreased productivity at school or work.
TREATMENT OF AR
Effective management of AR often requires a combination of avoidance measures, medication and allergen immunotherapy (AlT). The Allergic Rhinitis and its Impact on Asthma (ARIA) international workgroup recommends oral antihistamines or intranasal steroid sprays as the first line treatment in AR AIT is the second line treatment in those whom pharmacotherapy is ineffective, poorly tolerated or not desired. Its impact is more pronounced in those who are highly symptomatic.
ALLERGEN
IMMUNOTHERAPY (AIT) AIT is the only disease modifying treatment modality, unlike antihistamines or steroids. Its mechanism of action includes activation of lgG antibodies, regulatory T cells, mediators and cytokines that attenuate allergic inflammation. Clinical improvement can be observed as soon as a few weeks of administration. It has an added benefit of sustained symptom relief even after completion of treatment, which is typically 3 to 5 years. Good compliance to treatment is required for optimal results.

Allergic rhinitis (AR) is highly prevalent in Singapore. It occurs in about 40% of our population, making the prevalence of AR in Singapore amongst the highest in the world. It is also strongly associated with asthma and both conditions often coexist.
There are currently two approaches to AlT: subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT). The subcutaneous route is the traditional method, but it carries a small risk of anaphylaxis which can be life-threatening. The sublingual route is gaining in popularity due to the convenience of home administration as well as fewer and less severe adverse effects A recent multicenter randomised double-blind, placebo-controlled trial showed that HDM SLIT reduced AR symptoms and medication usage in patients with moderate to severe HDM-induced AR.
In 2017, we performed 884 SPT and 91 RAST tests, SPT is popular as it is a quick test, with results readily available after about 30 minutes. RAST is performed for those who are unable to be weaned off antihistamines.
In SLIT, the allergen extract is prepared in either a spray or tablet form. It is placed under the tongue for 1 to 2 minutes and then swallowed.
This is done daily over a course of 3 to 5 years to develop lasting immunity. The benefit of the tablet form is that it obviates the need for storage in the refrigerator.
SLIT has a good safety profile. Some of the side effects such as throat itch, local erythema or edema, which can be managed with pre-administration of antihistamines. It is suitable for children over the age of 5.
Based on a recent study on the use of SLIT in asthma patients, the 2017 Global Initiative for Asthma (GINA) guideline now recommends the addition of SLIT in adult patients with HDM-induced AR and allergic asthma who have frequent exacerbations despite inhaled corticosteroids, provided that the FEVI is more than 70% predicted.
NUH OTOLARYNGOLOGY (ENT) - ALLERGY CLINIC
Since 1985, we have a dedicated Otolaryngology (ENT) Allergy Clinic located within the ENT — Head & Neck Surgery Centre. This facility is a specialised clinical service comprising a team of doctors, allergy nurses and research scientists. The clinic provides evaluation and treatment for both adults and children with AR and other nasal conditions such as sinusitis and nasal polyps.
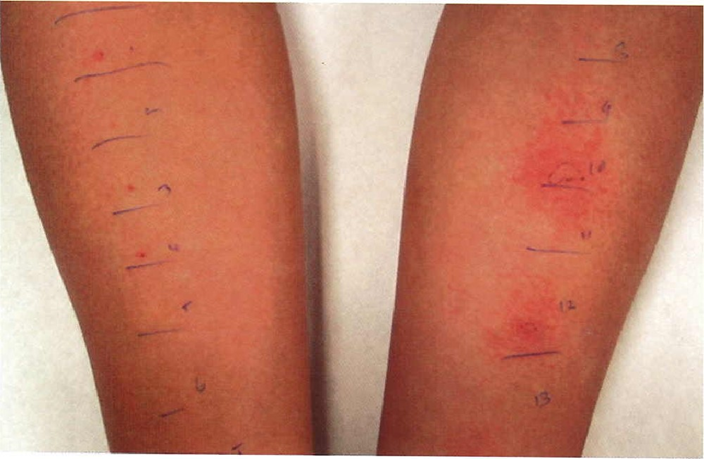
Figure 1: Skin prick test
The clinic offers a full range of diagnostic services ranging from skin prick test (SPT) (Figure 1), serum radioallergosorbent (RAST) blood test, intradermal test and acoustic rhinometry.

Figure 2: Allergy counselling performed by the nurse practitioner
Following identification of the offending allergens, our nurse practitioners will educate patients on the natural history of the condition and recommend appropriate avoidance measures to reduce allergen exposure (Figure 2).

For suitable candidates in whom medication are ineffective or poorly tolerated, or who do not wish to be on long-term medication, the option of AIT (Figure 3) is introduced. There are currently 28 patients undergoing SLIT therapy and 3 undergoing SCIT therapy. Amongst those undergoing SLIT, 70% of patients have reported improvement in their quality of life popular questionnaire scores, These patients undergoing AIT are continuously reviewed and monitored.

Comments